
Fibroids: 7 Facts To Know
These common uterine growths can cause significant symptoms and impede pregnancy, but effective treatments are available.

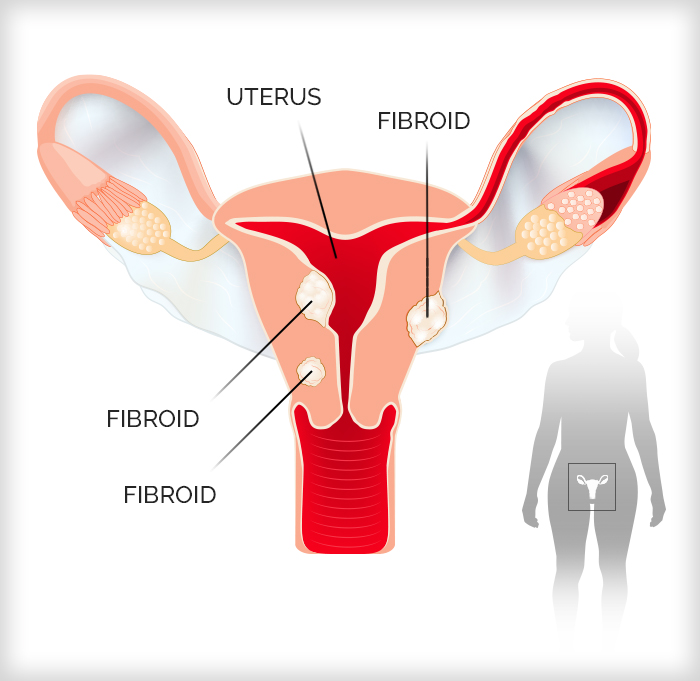
Fibroids — noncancerous growths of the uterus — are one of the most common health conditions people face during childbearing years. While not life-threatening, they can impact your quality of life. The good news? There are effective treatments available, including for those who want to have children in the future.
“Women with fibroids should know that there are options to help them address things like their heavy menstrual bleeding and the potential impact on fertility,” says Dr. Arnold P. Advincula, chief of the Division of Gynecologic Specialty Surgery at NewYork-Presbyterian/Columbia University Irving Medical Center.
Here, Dr. Advincula explains what you need to know about this condition, its symptoms, and the latest advances to treat it.
1. Fibroids can grow as big as a watermelon — or number in the dozens.
Fibroids, which are fueled by estrogen and progesterone, the hormones governing menstruation and ovulation, vary widely from one patient to another.
“Grapefruit size is about the standard that we see in the office, but there are patients who show up with watermelon-sized tumors in their belly,” says Dr. Advincula. “They look like they’re pregnant. They’re often frustrated by people walking up to them and asking when they’re due because their abdomen is so distended.”
Conversely, some patients have multiple smaller fibroids. It’s not unusual for doctors to find 60 or more of these growths. “The imaging of patients with this type of presentation makes the uterus look like it is full of tiny marbles,” Dr. Advincula says.
2. Fibroids can affect your quality of life.
Many people with fibroids feel no symptoms while others can experience discomfort or menstrual bleeding so heavy that it results in anemia or interferes with a patient’s work and lifestyle.
“When you need a super tampon and a super maxi pad to try to avoid an accident when you’re on your period, that’s not normal,” says Dr. Advincula. “Fortunately, there are treatment options to address these problems.”
Bowel and bladder symptoms, pelvic pain, and abdominal bloating are also common. Patients with fibroids may complain of having to urinate constantly, even when they have had only a small amount to drink.
“If the uterus is enlarged, it compresses the bladder and limits its capacity to hold fluid,” says Dr. Advincula. “Similarly, some women will complain of constipation because their pelvis is so full of fibroids that the bowel can’t function normally. Collectively, these are called bulk symptoms.”
3. Fibroids can throw a wrench into family planning.
Most people with fibroids can have a healthy pregnancy. However, fibroids can impact fertility and childbirth in several ways. For instance, they can affect the inner lining of the uterus, called the endometrial cavity, where menstruation originates and a fertilized egg implants.
“Once the endometrial cavity is disrupted by fibroids, it causes heavy menstrual bleeding, which makes it difficult to get pregnant,” Dr. Advincula says. “It’s almost impossible to conceive if you’re constantly having a period.” The distortion of the endometrial cavity also makes it harder for an embryo to implant.

Dr. Arnold Advincula
When pregnancy is successful, fibroids can continue to grow because of the influence of pregnancy hormones. “When women who have fibroids get pregnant, their fibroids can experience accelerated growth,” Dr. Advincula says.
Fibroid growth can result in pain, cause a miscarriage, or lead to early or obstructed labor requiring a cesarean section. “One of the most common referrals that we get are from fertility specialists doing in vitro fertilization (IVF),” Dr. Advincula says. “They realize that they can’t do IVF on a patient because they’ve got a fibroid impinging on the endometrial cavity or blocking access to the ovaries for egg retrievals.” Discuss with your doctor treatment options that address fertility issues.
4. Black women suffer the most from fibroids.
African American women have three times the risk for developing fibroids when compared with white women. By the time Black women enter menopause at around age 50, more than 80% of them have had fibroids, compared to about 70% of white women.
Black women tend to experience fibroids at an earlier age, have larger and more fast-growing fibroids, and feel more severe symptoms.
At the same time, disparities and biases can negatively affect Black patients’ ability to get appropriate fibroid treatments, Dr. Advincula says. “For instance, if you’re Black, you’re less likely to have a conservative fertility-sparing or minimally invasive option presented to you,” Dr. Advincula says. Minimally invasive procedures involve less pain and have a shorter recovery — two weeks or less, compared to six weeks with open procuedures.
5. Fibroids should be treated earlier rather than later.
Many complications of fibroids can be minimized by addressing them at an earlier stage, Dr. Advincula says. For instance, it’s more challenging to manage large fibroids in patients who wish to become pregnant.
Dr. Advincula says it’s important to weigh symptoms, the extent and location of fibroids, and an individual’s childbearing goals at the time of diagnosis to help avoid future problems. “Otherwise, you may end up at a point where all of a sudden it does compromise your fertility or you are having heavy menstrual bleeding that results in anemia,” he says.
Often, small fibroids — 2 or 3 centimeters in diameter — don’t require attention, depending on their location. “But when you’re looking at a fibroid that has grown to 7 or 8 centimeters, it could have implications,” Dr. Advincula says. If you have fibroids, your doctor will monitor them to see if they have grown or you need treatment.
6. Fibroid treatments are better than ever, and options have expanded.
“We now have a number of good alternatives that we can customize to meet the needs of most patients,” says Dr. Advincula. There is no one-size-fits-all treatment, he says. Instead, treatments are tailored to women’s medical needs and preferences, including the size and number of fibroids and whether the patient desires children.
Treatment often starts with symptom relief. Hormonal-based therapies, like birth control pills, can reduce bleeding. Over-the-counter pain relievers, like ibuprofen, can ease menstrual cramps. Other drugs, such as leuprolide (Lupron), can shrink fibroids by triggering temporary menopause and are often used before a patient proceeds with surgery. Oral drugs like the newer medication elagolix can control heavy bleeding caused by fibroids. It works by suppressing ovarian hormones which in turn can stop periods.
"We now have a number of good alternatives that we can customize to meet the needs of most patients."— Dr. Arnold Advincula
7. Fibroid procedures may preserve fertility.
Additional Resources
Learn more about uterine fibroid treatments at NewYork-Presbyterian.
Arnold Advincula, M.D., is an obstetrician-gynecologist and chief of the Division of Gynecologic Specialty Surgery at NewYork-Presbyterian/Columbia University Irving Medical Center and chief of gynecology at the Sloane Hospital for Women. He is also the Richard U. Levine Professor of Women’s Health and vice chair of women’s health in the Department of Obstetrics and Gynecology at Columbia University Vagelos College of Physicians and Surgeons. Dr. Advincula is a leader in minimally invasive surgical techniques and gynecologic robotic surgery. He has published and taught extensively in the area of minimally invasive surgery and has developed surgical instruments in use worldwide. Dr. Advincula has extensive experience in treating complex and challenging cases of endometriosis, uterine fibroids, and pelvic masses.